
The single document most likely to sink an otherwise solid SSDI claim is the Residual Functional Capacity assessment. Known as the RFC, this is where medical notes must be translated into precise, legally usable limitations. RFC errors now account for nearly half of initial SSDI denials.
The reason is blunt: adjudicators treat the RFC as the bridge between medicine and law. Vague language, missing functional details, or a mismatch between symptoms and specific work restrictions gives the Social Security Administration a lawful basis to deny. A chart note that says “limited” is not the same as a defensible, activity-based RFC that shows why full-time work is impossible.
In this post we will dismantle the RFC Trap. You will learn the exact functional data points adjudicators expect, the drafting mistakes that trigger denials, and a practical checklist to convert clinical records into a standards-compliant RFC. New to SSDI? Start with our guide, How to Apply for Disability Benefits (SSDI & SSI).
Key Takeaways:
-
The Residual Functional Capacity (RFC) assessment is a legal instrument, not merely a medical form, that the SSA uses to justify denial if it fails to strictly quantify your work limitations.
-
Avoid the language trap: the SSA requires quantified work restrictions (minutes, pounds, percentage of time off-task), not vague clinical statements like "chronic pain."
-
Claims often fail because the RFC neglects to address Non-Exertional Limitations (NELS) such as cognitive deficits, fatigue, or attendance issues which are critical for proving unemployability.
-
To win, your RFC must restrict your capacity below the Sedentary Work threshold, for example, by limiting standing to less than two hours or mandating unpredictable, frequent breaks.
-
Due to the necessity of cross-referencing all medical data against specific federal regulations, procedural compliance is best guaranteed by specialized, automated drafting assistance.
What is a Residual Functional Capacity (RFC) Assessment?
The Residual Functional Capacity (RFC) Assessment is the single most critical document in the SSA's five-step evaluation process for SSDI and SSI claims. It is a mandatory legal determination of the most work you can still do despite your proven medical impairments. Unlike a simple doctor's note, the RFC translates vague diagnoses into specific, quantified functional limitations. It measures your remaining capacity for sustained work across physical factors (lifting, standing, sitting) and mental factors (concentration, persistence, pace). The SSA uses the RFC to assign you an exertional level—Sedentary, Light, or Medium—and if the report fails to restrict you below the Sedentary level, your claim will almost certainly be denied, as the SSA will conclude you can perform some work in the national economy.
The Pivot Point: Understanding the SSA’s Five-Step Gauntlet
To appreciate the destructive power of a flawed RFC, you must first understand the SSA’s mandatory Five Step Sequential Evaluation Process. This process is not about compassion; it is a rigid legal screening. The RFC doesn’t come into play until the most critical, final steps.
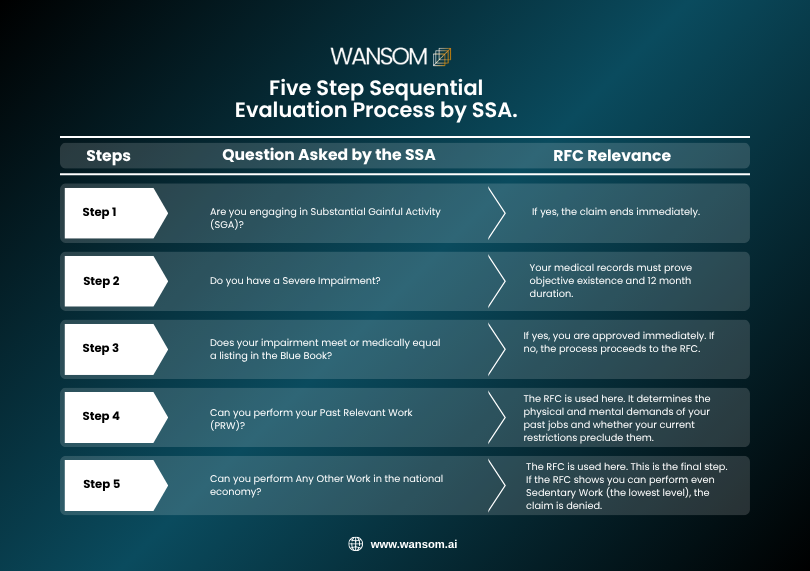
The move from Step 3 to Step 4 is the transition from a purely medical review (checking against the Blue Book) to a functional review. The RFC is the document that measures your remaining capacity your "residual function." This single form becomes the legal measuring tape the SSA uses to justify denying you at Step 4 or Step 5. If the RFC is flawed, it grants the SSA legal permission to claim you can still work.
The Trap: Why 50% of Functional Reports Fail the Legal Test
The fundamental reason for the RFC’s high failure rate is a catastrophic failure of communication and translation between two completely different fields: clinical medicine and federal disability law. Your physician is focused on your treatment and pain management; the SSA adjudicator is focused only on whether you fit a specific legal definition of an "unemployable person."
The result is a gap that only procedural compliance can bridge.
1. The Language Gap: Clinical vs. Functional Terminology
A physician’s notes are written in clinical language; they discuss diagnoses like "L4-L5 disc herniation" or "Generalized Anxiety Disorder." This is the language of treatment.
The SSA, however, requires functional language. They don't care what your diagnosis is; they care what your diagnosis prevents you from reliably doing eight hours a day, five days a week, week after week.
-
Clinical Statement: "Patient experiences severe, chronic lower back pain."
-
SSA Interpretation: This is subjective and non-specific. Does it prevent all work?
-
-
Functional Statement (RFC-Compliant): "Due to chronic L4-L5 radiculopathy, the patient cannot stand or walk for more than 15 minutes continuously or 1 hour total in an 8 hour workday, and can never lift more than 5 pounds. The patient requires the option to shift positions every 30 minutes, which is medically necessary."
-
SSA Interpretation: This is quantifiable, absolute, and job-preclusive. It severely restricts the range of Sedentary Work the claimant can perform.
-
The trap is set when the physician, acting with the best intentions, writes a vague, clinically accurate but functionally useless report that fails to use quantifiers (minutes, pounds, degrees of motion, percentage of time).
2. The Tyranny of the Checkbox Form
The official SSA forms or the generic third party forms often utilized by medical offices are inherently dangerous. They rely heavily on checkboxes and simple lines. While they appear comprehensive, they are deadly because they enforce brevity and discourage the necessary narrative explanation.
A physician, under time pressure, might check: "Limited to Light Work."
What the SSA sees: The applicant can lift 20 pounds occasionally and 10 pounds frequently, and can stand and walk for up to 6 hours. What the physician meant: The patient cannot perform their old job, but they still have some residual ability.
This single checkbox check destroys the entire claim because the SSA now concludes you are capable of Light Work, which exists in abundance in the national economy. Your claim, which was medically legitimate, is now administratively denied at Step 5.
The solution is that the RFC must be a narrative document, not merely a checked box. Every single limitation, especially non-exertional ones, must be fully explained and tied directly back to the specific objective medical evidence (OME) in the file (e.g., "The limit of lifting 5 pounds is directly due to the verified, measured 3/5 muscle strength in the left bicep documented on the EMG report dated [Date]").
3. The Failure to Address Non-Exertional Limitations
The most common denial reason is that the RFC focuses too much on physical limits (exertional) and completely neglects non-exertional limitations (NELS). NELS are often the true reason someone can't hold a job, yet they are the hardest to document and quantify.
Non-exertional limitations include:
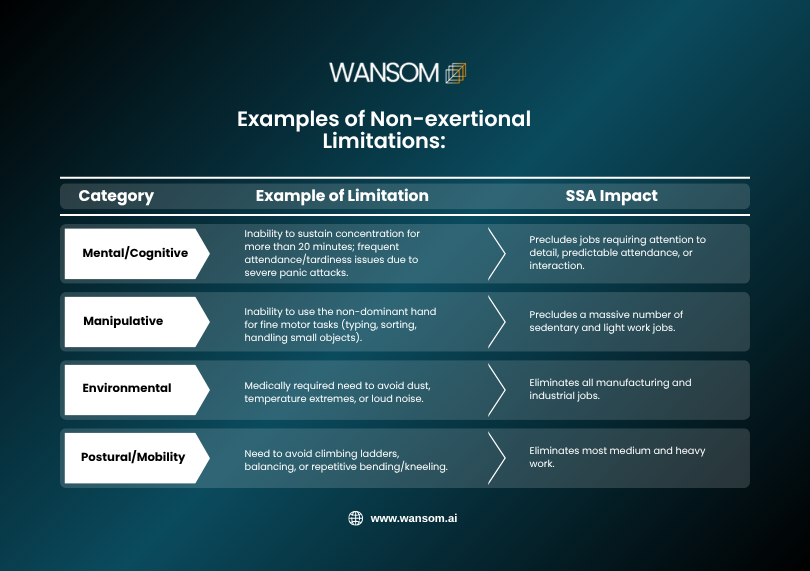
If the RFC only states you can't lift heavy boxes, the SSA will simply assign you to a sedentary job. However, if the RFC also states you have an unpredictable need to leave the workstation due to IBS flares or pain crises at least 3 times per day, no employer will hire you. The NELS are the ultimate, game winning factor, and their absence in the RFC is the trap.
Dissecting the Complexity: The Three Components of a Compliant RFC
To safely navigate the RFC process, you must be hyper-aware of the detailed questions the SSA is really asking in the report. A compliant RFC must systematically restrict the claimant from all five SSA work levels (Sedentary, Light, Medium, Heavy, Very Heavy).
1. The Physical RFC: Exertional Limitations
The physical RFC determines your maximum sustained ability to perform the eight primary physical demands of all work.
A. Lifting and Carrying (The Weight Limit)
The SSA divides work by how much you can lift frequently (up to 2/3 of the day) and occasionally (up to 1/3 of the day). Your doctor must specify absolute limits, supported by evidence of muscle weakness, joint destruction, or pain severity.
|
Work Level |
Occasionally Lift (1/3 Day) |
Frequently Lift (2/3 Day) |
|
Sedentary |
10 lbs |
Negligible (Less than 10 lbs) |
|
Light |
20 lbs |
10 lbs |
|
Medium |
50 lbs |
25 lbs |
|
Heavy/Very Heavy |
100+ lbs |
50+ lbs |
The Trap: If your doctor only checks "Limited to 10 pounds," the SSA will conclude you can perform Sedentary Work, which typically requires lifting less than 10 pounds frequently. The RFC must specify restrictions below the Sedentary threshold (e.g., "Cannot lift or carry more than 5 pounds occasionally.").
B. Standing and Walking (The Mobility Limit)
The core SSA definition of Sedentary Work requires the ability to stand and walk occasionally (typically 2 hours total in 8 hours), but primarily sitting.
The Trap: Many doctors indicate "Needs to sit," but fail to specify the standing/walking limit. If your RFC only restricts you to standing/walking for 4 hours total, the SSA rules you capable of Light Work. To be restricted to Sedentary Work, the RFC must specify standing/walking limits of 2 hours or less total in 8 hours. To win the claim at this level, the RFC must show an additional limitation, such as the need to shift positions at will or unpredictable rest breaks that an employer cannot accommodate.
C. Postural and Manipulative Limits (Non-Exertional)
These sections determine the range of motion you retain. They are powerful claim winners because they eliminate massive categories of jobs that require even minimal movement.
-
Handling, Fingering, Feeling: If your doctor indicates an inability to use your hands for repetitive small motions (due to neuropathy, carpal tunnel, arthritis, etc.), you are precluded from most sedentary work, which often involves typing and paperwork.
-
Climbing, Balancing, Kneeling: The doctor must specify if you can never perform these actions. If the RFC fails to restrict these, the SSA will assume you are capable of occupations that demand them.
2. The Mental RFC: The Cognitive Complexity
Mental impairment claims require a rigorous, almost mathematical approach because the SSA uses the Four Corners of Functioning to evaluate mental health. The adjudicator must assess your ability to function across these four key areas:
A. Understanding and Memory
This assesses your ability to learn new tasks, remember work locations, and follow one, two, or multi step instructions.
Compliant RFC Language: "Due to documented cognitive deficits (confirmed by the WAIS-IV score of [score] in working memory), the claimant can only reliably remember and carry out simple, non-detailed, one-or-two step instructions. They are incapable of following detailed written procedures or recalling complex instructions over a full workday."
B. Sustained Concentration and Persistence
This is the single most important mental domain. It measures your ability to work at a consistent pace and sustain attention through an eight hour workday without needing unscheduled, excessive breaks.
The Trap: Many claimants suffer from severe fatigue, "brain fog," or intrusive mental symptoms (like racing thoughts from anxiety or PTSD flashbacks) that cause them to lose pace. The RFC must explicitly state that the claimant is predicted to experience off task behavior or unscheduled breaks amounting to more than 15% of the workday. If you are off task for 15% of the day, you are not reliably competitive in the job market, and the claim should be approved.
C. Social Interaction
This measures your ability to work with supervisors, coworkers, and the public.
Compliant RFC Language: "Due to extreme paranoia and documented symptoms of social avoidance, the claimant is limited to work involving no contact with the public and only brief, occasional, non-supervisory contact with coworkers. They would be unable to tolerate performance critique or adjust to sudden changes in supervisory style."
D. Adaptation and Management
This assesses your ability to handle routine work stress, adapt to changes in the work setting (even minor ones), and manage a regular schedule.
The Trap: The SSA assumes that all people can handle stress. The RFC must be explicit that the claimant's underlying medical or mental health condition (e.g., Severe Bi-polar Disorder or uncontrolled pain) makes them medically unable to tolerate even low levels of routine work stress, leading to emotional breakdowns, exacerbation of physical symptoms, or a complete inability to attend work for extended periods.
3. The Environmental and Other Limitations
The RFC must cover any limitations that preclude work environments. These are often the easiest restrictions to prove with objective medical evidence but are frequently overlooked.
-
Avoidance of Hazards: Due to anti-seizure medication side effects or vestibular issues, the claimant is restricted from working at unprotected heights or near dangerous, moving machinery. This immediately precludes all factory and manual labor jobs.
-
Temperature Extremes: For claimants with conditions like Multiple Sclerosis (MS) or specific chronic lung conditions, the RFC must state a medical necessity to avoid heat, cold, or high humidity.
-
Fumes and Dust: For claimants with asthma, COPD, or severe allergic sensitivities, the RFC must mandate avoidance of concentrated dust, fumes, poor ventilation, and other respiratory irritants. This is a powerful restriction that rules out most manufacturing and industrial environments, even for sedentary positions.
Conclusion
You now understand the sheer complexity of the RFC. It requires your doctor to be a medical expert, a legal translator, and an expert witness all at once. The form demands absolute precision, perfect consistency with your medical file, and the use of specific, legally restrictive language. This is simply not a task that can be left to an overworked physician or handled by the claimant alone, which is precisely why the denial rate is 50% at the RFC stage.
Your file must systematically convince the SSA that your documented limitations are so severe and pervasive that no job not even the simplest, most sedentary job can accommodate you reliably.
The Impossibility of Perfect Compliance
Manually gathering, synthesizing, and translating thousands of pages of disparate medical records into a single, cohesive, 100% compliant RFC is nearly impossible for a layperson. Even experienced disability lawyers spend countless hours reviewing files for these exact, costly inconsistencies.
The typical process involves:
-
Identifying the exact medical facts.
-
Correlating those facts to the SSA’s specific regulatory definitions (the Code of Federal Regulations).
-
Drafting language that restricts work capacity below the Sedentary level.
-
Ensuring every single limitation is backed by an explicit date and source in your medical records.
One missed detail, one vague quantifier, one failure to address non-exertional limits and the SSA has the legal justification it needs to deny your claim. You risk wasting months, if not years, in the appeals process.
Your Next Step: Guaranteeing Compliance
You are facing a legal and administrative hurdle, not just a medical one. You have the medical proof; now you need the procedural precision. Do not allow your legitimate disability claim to be undone by a technical flaw in a single, critical form.

The time for anxiety is over; the time for action is now.
Eliminate the risk. Guarantee procedural compliance for the most important document in your SSDI claim. Click below to access the Wansom AI Drafting Engine and ensure your Residual Functional Capacity report is undeniable.
Access the Wansom AI Drafting Engine Now to Draft Your Compliant RFC
Jump to:
-
6 Types of Medical Evidence the SSA Cannot Ignore in Your Disability Claim
-
How to Draft a Personal Injury Settlement Agreement: Complete Guide + Free Template
Leave a Reply